Pharmacotherapeutic group: Anti-inflammatory and antirheumatic products, non-steroids, coxibs.
ATC code: M01 AH05.
Pharmacology: Pharmacodynamics: Mechanism of Action: Etoricoxib is an oral, selective cyclo-oxygenase-2 (COX-2) inhibitor within the clinical dose range.
Across clinical pharmacology studies, etoricoxib produced dose-dependent inhibition of COX-2 without inhibition of COX-1 at doses up to 150 mg daily. Etoricoxib did not inhibit gastric prostaglandin synthesis and had no effect on platelet function.
Cyclooxygenase is responsible for generation of prostaglandins. Two isoforms, COX-1 and COX-2, have been identified. COX-2 is the isoform of the enzyme that has been shown to be induced by pro-inflammatory stimuli and has been postulated to be primarily responsible for the synthesis of prostanoid mediators of pain, inflammation, and fever. COX-2 is also involved in ovulation, implantation and closure of the ductus arteriosus, regulation of renal function, and central nervous system functions (fever induction, pain perception and cognitive function). It may also play a role in ulcer healing. COX-2 has been identified in tissue around gastric ulcers in man but its relevance to ulcer healing has not been established.
Clinical efficacy and safety: Efficacy: In patients with osteoarthritis (OA), etoricoxib 60 mg once daily provided significant improvements in pain and patient assessments of disease status. These beneficial effects were observed as early as the second day of therapy and maintained for up to 52 weeks. Studies with etoricoxib 30 mg once daily demonstrated efficacy superior to placebo over a 12 week treatment period (using similar assessments as the previously mentioned studies). In a dose ranging study, etoricoxib 60 mg demonstrated significantly greater improvement than 30 mg for all 3 primary endpoints over 6 weeks of treatment. The 30 mg dose has not been studied in osteoarthritis of hands.
In patients with rheumatoid arthritis, etoricoxib 60 mg and 90 mg once daily both provided significant improvements in pain, inflammation, and mobility. In studies evaluating the 60 mg and 90 mg dose, these beneficial effects were maintained over the 12-week treatment periods. In a study evaluating the 60 mg dose compared to the 90 mg dose, etoricoxib 60 mg once daily and 90 mg once daily were both more effective than placebo. The 90 mg dose was superior to the 60 mg dose for Patient Global Assessment of Pain (0-100 mm visual analogue scale), with an average improvement of -2.71 mm (95 % CI: -4.98 mm, -0.45 mm).
In patients experiencing attacks of acute gouty arthritis, etoricoxib 120 mg once daily over an eight-day treatment period, relieved moderate to extreme joint pain and inflammation comparable to indomethacin 50 mg three times daily. Pain relief was observed as early as four hours after initiation of treatment.
In patients with ankylosing spondylitis, etoricoxib 90 mg once daily provided significant improvements in spine pain, inflammation, stiffness and function. The clinical benefit of etoricoxib was observed as early as the second day of therapy after initiation of treatment and was maintained throughout the 52-week treatment period. In a second study evaluating the 60 mg dose compared to the 90 mg dose, etoricoxib 60 mg daily and 90 mg daily demonstrated similar efficacy compared to naproxen 1,000 mg daily. Among inadequate responders to 60mg daily for 6 weeks, dose escalation to 90 mg daily improved spinal pain intensity score (0-100 mm visual analogue scale) compared to continuing on 60 mg daily, with an average improvement of -2.70 mm (95 % CI: -4.88 mm, -0.52 mm).
In a clinical study evaluating postoperative dental pain, etoricoxib 90 mg was administered once daily for up to three days. In the subgroup of patients with moderate pain at baseline, etoricoxib 90 mg demonstrated a similar analgesic effect to that of ibuprofen 600 mg (16.11 vs. 16.39; P=0.722), and greater than that of paracetamol/codeine 600 mg/60 mg (11.00; P<0.001) and placebo (6.84; P<0.001) as measured by total pain relief over the first 6 hours (TOPAR6). The proportion of patients reporting rescue medication usage within the first 24 hours of dosing was 40.8 % for etoricoxib 90 mg, 25.5 % for ibuprofen 600 mg Q6h, and 46.7 % for paracetamol/codeine 600 mg/60 mg Q6h compared to 76.2 % for placebo. In this study, the median onset of action (perceptible pain relief) of 90 mg etoricoxib was 28 minutes after dosing.
Safety: Multinational Etoricoxib and Diclofenac Arthritis Long-term (MEDAL) Programme: The MEDAL Programme was a prospectively designed Cardiovascular (CV) Safety Outcomes Programme of pooled data from three randomized, double-blind active comparator controlled trials, the MEDAL study, EDGE II and EDGE.
The MEDAL Study, was an endpoint driven CV Outcomes study in 17,804 patients with osteoarthritis and 5,700 patients with rheumatoid arthritis treated with etoricoxib 60 mg (osteoarthritis) or 90 mg (osteoarthritis and rheumatoid arthritis) or diclofenac 150 mg daily for a mean period of 20.3 months (maximum of 42.3 months, median 21.3 months). In this trial, only serious adverse events and discontinuations due to any adverse events were recorded.
The EDGE and EDGE II studies compared the gastrointestinal tolerability of etoricoxib versus diclofenac. The EDGE study included 7,111 osteoarthritis patients treated with a dose of etoricoxib 90 mg daily (1.5 times the dose recommended for osteoarthritis) or diclofenac 150 mg daily for a mean period of 9.1 months (maximum 16.6 months, median 11.4 months). The EDGE II study included 4,086 rheumatoid arthritis patients treated with etoricoxib 90 mg daily or diclofenac 150 mg daily for a mean period of 19.2 months (maximum 33.1 months, median 24 months).
In the pooled MEDAL Programme, 34,701 patients with osteoarthritis or rheumatoid arthritis were treated for a mean duration of 17.9 months (maximum 42.3 months, median 16.3 months) with approximately 12,800 patients receiving treatment for more than 24 months. Patients enrolled in the Programme had a wide range of cardiovascular and gastrointestinal risk factors at baseline. Patients with a recent history of myocardial infarction, coronary artery bypass grafting or percutaneous coronary intervention within 6 months preceding enrolment were excluded. Use of gastroprotective agents and low dose acetylsalicylic acid were permitted in the studies.
Overall Safety: There was no significant difference between etoricoxib and diclofenac in the rate of cardiovascular thrombotic events. Cardiorenal adverse events were observed more frequently with etoricoxib than with diclofenac, and this effect was dose-dependent (see specific results as follows). Gastrointestinal and hepatic adverse events were observed significantly more frequently with diclofenac than etoricoxib. The incidence of adverse experiences in EDGE and EDGE II and of adverse experiences considered serious or resulting in discontinuation in the MEDAL study was higher with etoricoxib than diclofenac.
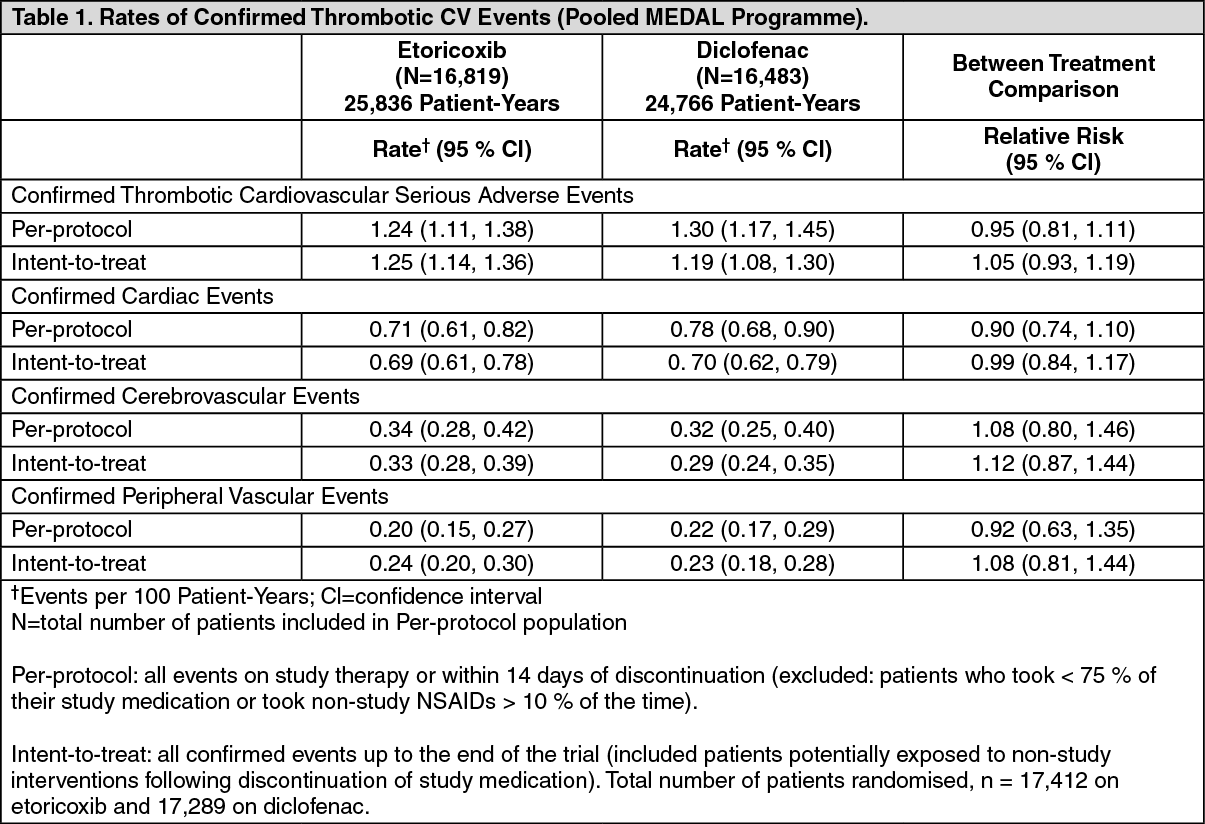
Cardiovascular safety results: The rate of confirmed thrombotic cardiovascular serious adverse events (consisting of cardiac, cerebrovascular, and peripheral vascular events) was comparable between etoricoxib and diclofenac, and data are summarized in the following table. There were no statistically significant differences in thrombotic event rates between etoricoxib and diclofenac across all subgroups analysed including patient categories across a range of baseline cardiovascular risk. When considered separately, the relative risks for confirmed thrombotic cardiovascular serious adverse events with etoricoxib 60 mg or 90 mg compared with diclofenac 150 mg were similar. (See Table 1.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
CV mortality, as well as overall mortality, was similar between the etoricoxib and diclofenac treatment groups.
Cardiorenal Events: Approximately 50 % of patients enrolled in the MEDAL study had a history of hypertension at baseline. In the study, the incidence of discontinuations due to hypertension-related adverse events was statistically significantly higher for etoricoxib than for diclofenac. The incidence of congestive heart failure adverse events (discontinuations and serious events) occurred at similar rates on etoricoxib 60 mg compared to diclofenac 150 mg but was higher for etoricoxib 90 mg compared to diclofenac 150 mg (statistically significant for 90 mg etoricoxib vs. 150 mg diclofenac in MEDAL osteoarthritis cohort). The incidence of confirmed congestive heart failure adverse events (events that were serious and resulted in hospitalisation or a visit to an emergency department) was non-significantly higher with etoricoxib than diclofenac 150 mg, and this effect was dose-dependent. The incidence of discontinuations due to oedema-related adverse events was higher for etoricoxib than diclofenac 150 mg, and this effect was dose-dependent (statistically significant for etoricoxib 90 mg, but not for etoricoxib 60 mg).
The cardiorenal results for EDGE and EDGE II were consistent with those described for the MEDAL Study.
In the individual MEDAL Programme studies, for etoricoxib (60 mg or 90 mg), the absolute incidence of discontinuation in any treatment group was up to 2.6 % for hypertension, up to 1.9 % for oedema, and up to 1.1 % for congestive heart failure, with higher rates of discontinuation observed with etoricoxib 90 mg than etoricoxib 60 mg.
MEDAL Programme Gastrointestinal (GI) Tolerability Results: A significantly lower rate of discontinuations of treatment for any clinical (e.g., dyspepsia, abdominal pain, ulcer) GI adverse event was observed with etoricoxib compared with diclofenac within each of the three component studies of the MEDAL Programme. The rates of discontinuations due to adverse clinical GI events per hundred patient-years over the entire period of study were as follows: 3.23 for etoricoxib and 4.96 for diclofenac in the MEDAL Study; 9.12 with etoricoxib and 12.28 with diclofenac in the EDGE study; and 3.71 with etoricoxib and 4.81 with diclofenac in the EDGE II study.
MEDAL Programme Gastrointestinal Safety Results: Overall upper GI events were defined as perforations, ulcers and bleeds (PUBs). The subset of overall upper GI events considered complicated included perforations, obstructions, and complicated bleeding; the subset of upper GI events considered uncomplicated included uncomplicated bleeds and uncomplicated ulcers. A significantly lower rate of overall upper GI events was observed with etoricoxib compared to diclofenac. There was no significant difference between etoricoxib and diclofenac in the rate of complicated events. For the subset of upper GI haemorrhage events (complicated and uncomplicated combined), there was no significant difference between etoricoxib and diclofenac. The upper GI benefit for etoricoxib compared with diclofenac was not statistically significant in patients taking concomitant low-dose acetylsalicylic acid (approximately 33 % of patients).
The rates per hundred patient-years of confirmed complicated and uncomplicated upper GI clinical events (perforations, ulcers and bleeds [PUBs]) were 0.67 (95 % CI 0.57, 0.77) with etoricoxib and 0.97 (95 % CI 0.85, 1.10) with diclofenac, yielding a relative risk of 0.69 (95 % CI 0.57, 0.83).
The rate for confirmed upper GI events in elderly patients was evaluated and the largest reduction was observed in patients ≥ 75 years of age (1.35 [95 % CI 0.94, 1.87] vs. 2.78 [95 % CI 2.14, 3.56] events per hundred patient-years for etoricoxib and diclofenac, respectively.
The rates of confirmed lower GI clinical events (small or large bowel perforation, obstruction, or haemorrhage, [POBs]) were not significantly different between etoricoxib and diclofenac.
MEDAL Programme Hepatic Safety Results: Etoricoxib was associated with a statistically significantly lower rate of discontinuations due to hepatic-related adverse experiences than diclofenac. In the pooled MEDAL Programme, 0.3 % of patients on etoricoxib and 2. 7 % of patients on diclofenac discontinued due to hepatic-related adverse experiences. The rate per hundred patient-years was 0.22 on etoricoxib and 1.84 for diclofenac (p-value was < 0.001 for etoricoxib vs. diclofenac). However, most hepatic adverse experiences in the MEDAL Programme were non-serious.
Additional Thrombotic Cardiovascular Safety Data: In clinical studies excluding the MEDAL Programme Studies, approximately 3,100 patients were treated with etoricoxib ≥ 60 mg daily for 12 weeks or longer. There was no discernible difference in the rate of confirmed serious thrombotic cardiovascular events between patients receiving etoricoxib ≥ 60 mg, placebo, or non-naproxen NSAIDs. However, the rate of these events was higher in patients receiving etoricoxib compared with those receiving naproxen 500 mg twice daily. The difference in antiplatelet activity between some COX-1 inhibiting NSAIDs and selective COX-2 inhibitors may be of clinical significance in patients at risk of thrombo-embolic events. Selective COX-2 inhibitors reduce the formation of systemic (and therefore possibly endothelial) prostacyclin without affecting platelet thromboxane. The clinical relevance of these observations has not been established.
Additional Gastrointestinal Safety Data: In two 12-week double-blind endoscopy studies, the cumulative incidence of gastroduodenal ulceration was significantly lower in patients treated with etoricoxib 120 mg once daily than in patients treated with either naproxen 500 mg twice daily or ibuprofen 800 mg three times daily. Etoricoxib had a higher incidence of ulceration as compared to placebo.
Renal Function Study in the Elderly: A randomized, double-blind, placebo-controlled, parallel-group study evaluated the effects of 15 days of treatment of etoricoxib (90 mg), celecoxib (200 mg bid), naproxen (500 mg bid) and placebo on urinary sodium excretion, blood pressure, and other renal function parameters in subjects 60 to 85 years of age on a 200-mEq/day sodium diet.
Etoricoxib, celecoxib, and naproxen had similar effects on urinary sodium excretion over the 2 weeks of treatment. All active comparators showed an increase relative to placebo with respect to systolic blood pressures; however, etoricoxib was associated with a statistically significant increase at Day 14 when compared to celecoxib and naproxen (mean change from baseline for systolic blood pressure: etoricoxib 7.7 mmHg, celecoxib 2.4 mmHg, naproxen 3.6 mmHg).
Pharmacokinetics: Absorption: Orally administered etoricoxib is well absorbed. The absolute bioavailability is approximately 100 %. Following 120 mg once-daily dosing to steady state, the peak plasma concentration (geometric mean C
max = 3.6 μg/ml) was observed at approximately 1 hour (T
max) after administration to fasted adults. The geometric mean area under the curve (AUC
0-24hr) was 37.8 μg·hr/ml. The pharmacokinetics of etoricoxib are linear across the clinical dose range.
Dosing with food (a high-fat meal) had no effect on the extent of absorption of etoricoxib after administration of a 120 mg dose. The rate of absorption was affected, resulting in a 36 % decrease in C
max and an increase in T
max by 2 hours. These data are not considered clinically significant. In clinical trials, etoricoxib was administered without regard to food intake.
Distribution: Etoricoxib is approximately 92 % bound to human plasma protein over the range of concentrations of 0.05 to 5 μg/ml. The volume of distribution at steady state (V
dss) was approximately 1,201 in humans.
Etoricoxib crosses the placenta in rats and rabbits, and the blood-brain barrier in rats.
Biotransformation: Etoricoxib is extensively metabolised with < 1 % of a dose recovered in urine as the parent active substance. The major route of metabolism to form the 6'-hydroxymethyl derivative is catalysed by CYP enzymes. CYP3A4 appears to contribute to the metabolism of etoricoxib
in vivo.
In vitro studies indicate that CYP2D6, CYP2C9, CYP1A2 and CYP2C19 also can catalyse the main metabolic pathway, but their quantitative roles
in vivo have not been studied.
Five metabolites have been identified in man. The principal metabolite is the 6'-carboxylic acid derivative of etoricoxib formed by further oxidation of the 6'-hydroxymethyl derivative. These principal metabolites either demonstrate no measurable activity or are only weakly active as COX-2 inhibitors. None of these metabolites inhibit COX- 1.
Elimination: Following administration of a single 25 mg radiolabeled intravenous dose of etoricoxib to healthy subjects, 70 % of radioactivity was recovered in urine and 20 % in faeces, mostly as metabolites. Less than 2 % was recovered as unchanged active substance.
Elimination of etoricoxib occurs almost exclusively through metabolism followed by renal excretion. Steady state concentrations of etoricoxib are reached within seven days of once daily administration of 120 mg, with an accumulation ratio of approximately 2, corresponding to a half-life of approximately 22 hours. The plasma clearance after a 25 mg intravenous dose is estimated to be approximately 50 ml/min.
Characteristics in patients: Elderly patients: Pharmacokinetics in the elderly (65 years of age and older) are similar to those in the young.
Gender: The pharmacokinetics of etoricoxib are similar between men and women.
Hepatic impairment: Patients with mild hepatic dysfunction (Child-Pugh score 5-6) administered etoricoxib 60 mg once daily had an approximately 16 % higher mean AUC as compared to healthy subjects given the same regimen. Patients with moderate hepatic dysfunction (Child-Pugh score 7-9) administered etoricoxib 60 mg every other day had similar mean AUC to the healthy subjects given etoricoxib 60 mg once daily; etoricoxib 30 mg once daily has not been studied in this population. There are no clinical or pharmacokinetic data in patients with severe hepatic dysfunction (Child-Pugh score ≥ 10). (See Dosage & Administration and Contraindications.)
Renal impairment: The pharmacokinetics of a single dose of etoricoxib 120 mg in patients with moderate to severe renal insufficiency and patients with end-stage renal disease on haemodialysis were not significantly different from those in healthy subjects. Haemodialysis contributed negligibly to elimination (dialysis clearance approximately 50 ml/min). (See Contraindications and Precautions.)
Paediatric patients: The pharmacokinetics of etoricoxib in paediatric patients (<12 years old) have not been studied.
In a pharmacokinetic study (n=16) conducted in adolescents (aged 12 to 17) the pharmacokinetics in adolescents weighing 40 to 60 kg given etoricoxib 60 mg once daily and adolescents > 60 kg given etoricoxib 90 mg once daily were similar to the pharmacokinetics in adults given etoricoxib 90 mg once daily. Safety and effectiveness of etoricoxib in paediatric patients have not been established (see Dosage & Administration).
Toxicology: Preclinical safety data: In preclinical studies, etoricoxib has been demonstrated not to be genotoxic. Etoricoxib was not carcinogenic in mice. Rats developed hepatocellular and thyroid follicular cell adenomas at >2-times the daily human dose [90 mg] (based on systemic exposure) when dosed daily for approximately two years. Hepatocellular and thyroid follicular cell adenomas observed in rats are considered to be a consequence of rat-specific mechanism related to hepatic CYP enzyme induction. Etoricoxib has not been shown to cause hepatic CYP3A enzyme induction in humans.
In the rat, gastrointestinal toxicity of etoricoxib increased with dose and exposure time. In the 14-week toxicity study, etoricoxib caused gastrointestinal ulcers at exposures greater than those seen in man at the therapeutic dose. In the 53- and 106-week toxicity study, gastrointestinal ulcers were also seen at exposures comparable to those seen in man at the therapeutic dose. In dogs, renal and gastrointestinal abnormalities were seen at high exposures.
Etoricoxib was not teratogenic in reproductive toxicity studies conducted in rats at 15 mg/kg/day (this represents approximately 1.5 times the daily human dose [90 mg] based on systemic exposure). In rabbits, a treatment related increase in cardiovascular malformations was observed at exposure levels below the clinical exposure at the daily human dose (90 mg). However no treatment-related external or skeletal foetal malformations were observed. In rats and rabbits, there was a dose dependent increase in post implantation loss at exposures greater than or equal to 1.5 times the human exposure (see Contraindications and Use in Pregnancy & Lactation).
Etoricoxib is excreted in the milk of lactating rats at concentrations approximately two-fold those in plasma. There was a decrease in pup body weight following exposure of pups to milk from dams administered etoricoxib during lactation.


 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
 Sign Out
Sign Out
